Introduction: Spinal cord injury (SCI) is a devastating disease characterized by extensive cellular death, axonal disruption and scar formation, leading to lifelong disability, muscle spasms, sensory deficits and autonomic disturbances. Currently, no definitive therapy has been established to fundamentally improve neurological deficits in late chronic SCI (disease duration >1 year), which is the most prevalent among SCI patients. Transplantation of human umbilical cord mesenchymal stem cells (hUC-MSCs) is a promising therapeutic alternative and pilot studies have demonstrated that hUC-MSCs can potentially improve neurological dysfunction with minimal adverse events. However, compared with other phase of SCI, neurological dysfunction in late chronic SCI is more challenging to recover, as the severity of SCI tends to stabilize at one year after the initial injury. For these reasons, this clinical study aims to evaluate the safety and efficacy of subarachnoid transplantation of hUC-MSCs in patients with late chronic SCI.
Methods and Analysis: This is a prospective, multicenter, open-label, single-arm clinical study involving 43 adult patients with late chronic SCI. Participants will receive four consecutive subarachnoid infusions of hUC-MSCs (1.0×106 cells/kg), and will be regularly follow-up for four times, scheduled at 1, 3, 6, and 12 months after final hUC-MSCs transplantation. Safety will be assessed through the incidence and severity of adverse events (AEs) and serious adverse events (SAEs). Efficacy will be evaluated primarily by changes in the American Spinal Injury Association (ASIA) total score at 12 months post final transplantation. Secondary endpoints include ASIA impairment scale (AIS), Spinal Cord Independence Measure-III, muscle spasms, bladder and bowel function, and neurophysiological assessments.
Ethics and Dissemination: Ethical approval was obtained from the Institutional Ethics Committee of the Third Affiliated Hospital of Sun Yat-sen University and West China Hospital. Written informed consent will be obtained from all participants. This clinical study strictly adheres to the Declaration of Helsinki and Good Clinical Practice guidelines. Results will be disseminated through peer-reviewed publications and conference presentations, ensuring transparency and broad dissemination of findings.
STRENGTHS AND LIMITATIONS OF THIS STUDY
The choice of a single-arm design is particularly appropriate for late chronic SCI, where the condition has stabilized and participants might be hesitant about receiving a placebo.
Extensive safety evaluations, including in vitro and in vivo assays, rigorous microbiological testing, and continuous monitoring of adverse events, provide comprehensive insights into the safety profile of hUC-MSCs.
This study employs a wide range of outcome measures, and this in-depth evaluation provides a overall view of the efficacy and impact of hUC-MSC transplantation on various aspects of SCI recovery.
This study specifically targets late chronic SCI patients, which, while addressing an important unmet need, limits the applicability of the findings to other phases of SCI.
Given the open-label design of the study, both participants and investigators are aware of the intervention, which may introduce subjective bias.
INTRODUCTION
Spinal cord injury (SCI) is a devastating condition resulting in permanent neurological deficits due to primary mechanical damage and secondary pathological cascades1. SCI patients often suffer from lifelong disability, muscle spasms, sensory deficits, autonomic disturbances, as well as bowel and bladder incontinence2–4. Recent evident has shown that the incidence of various types of SCI remains high on a global scale5. The majority of SCI victims are young patients, who are at the time of working age6. As a result of that, SCI not only affects the physical and psychological health of those patients, but also bring huge economic burden to their families, as well as the society7. Despite current interventions, such as anti-inflammatory therapy, surgical decompression, regenerative medicine, and physical rehabilitation, treatment outcomes remain unsatisfactory, particularly for chronic SCI8,9.
In recent years, cell-based therapy advanced rapidly and had significant progress in treating SCI10–14. Human umbilical cord mesenchymal stem cells (hUC-MSCs) are considered a promising therapeutic candidate for intractable SCI due to numerous advantages, including paracrine ability15, homing capacity16, low immunogenicity17, and anti-fibrosis activity18. These advantages make it becomes a highly suitable candidate for SCI treatment19–25. Our preclinical studies26 using a rat SCI model demonstrated that subarachnoid transplantation of hUC-MSCs had minimal risk and offered significant benefits. However, high-quality data from well-designed studies are still lacking.
Among different transplantation routes, it has been proven that intrathecal delivery results in significantly better cell engraftment and tissue sparing, as well as a reduced host immune response27,28. Additionally, studies have reported that intrathecal administration of stem cells leads to better functional recovery when compared with other methods of cellular delivery22. Therefore, minimally invasive subarachnoid administration is considered the best approach for hUC-MSCs delivery.
Late chronic SCI, defined in this study as injury lasting more than one year, represents the largest patient subgroup and presents unique therapeutic challenges29. While our team has previously initiated a clinical trial using hUC-MSCs for early chronic SCI, late chronic SCI has been less explored and is considered more refractory to treatment30. For these reasons, this study adopts a prospective, open-label, single-arm design to evaluate subarachnoid transplantation of allogeneic hUC-MSCs in patients with late chronic SCI. This design ensures all participants receive the intervention, minimizing psychological barriers related to placebo assignment and aligning with patient expectations for potential recovery.
To the best of our knowledge, this will be the first well-designed study to evaluate safety and efficacy of hUC-MSCs in treating late chronic SCI, which is the most prevalent among SCI patients.
METHODS AND ANALYSIS
Study objective, design and setting
This project focuses on late chronic SCI that has a disease duration between 14-60 days and conducts a prospective clinical study to clarify clinical safety and efficacy of hUC-MSCs in treating it.
This multicenter, single-arm, open-label clinical study was registered with ClinicalTrials.gov on April 12, 2018 (registration No. NCT03505034). The revised study protocol (Protocol version 6.0) was released on December 27, 2021. The recruitment of participants started on 21 July 2020.
As for sample size estimation, a two-sided one-sample t-test was used. Based on the results of the preliminary clinical study, the standard difference of the American Spinal Injury Association (ASIA) total score difference between pre-treatment and post-treatment was 24. According to expert consensus from the spine surgery, rehabilitation and neurology departments, a minimum improvement of 12 in ASIA total score was believed to have clinical significance. Hence, a sample size of 34 could achieve 80% power to detect ASIA total score difference of 12 with a significance level of 0.05. The maximum possible dropout rate during follow-up was considered to be 20%. Therefore, 43 participants would be enough to support the sample size required for this study.
To expedite the recruitment of participants and enhance the generalizability of study outcomes while minimizing potential bias, this clinical study is performed at two hospitals in China. The initiating sponsor and coordinator is the Third Affiliated Hospital of Sun Yat-sen University (Guangzhou, China). The other participant is West China Hospital of Sichuan University (Chengdu, China). These two hospitals were located in southeastern, and western parts of China. The present study protocol is organized according to the Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT) checklist31,32.
Recruitment and eligibility criteria of participants
Patients will be recruited from two hospitals in China. Written informed consents that have been approved by institutional ethics committees will be obtained from the patients before enrollment or any study-specific procedures.
The inclusion criteria are as follows:
1. Complete or incomplete SCI: American Spinal Injury Association Impairment Scale (AIS) A-D.
2. Aged between 18 and 65 years old.
3. Duration of SCI is more than 12 months (the late chronic phase).
4. SCI induced by traumatic factors such as fall from height, motor vehicle accident, and violent injury.
5. Have voluntarily signed and dated an informed consent form after the nature of the clinical study was explained and participants had the opportunity to ask any question.
6. Agree to undergo regular follow-up for 12 months after treatment completion.
All of the above conditions must be satisfied for any participant to be included in this clinical study.
The exclusion criteria are as follows:
1. With ankylosing spondylitis.
2. With malignant tumors.
3. With neurodegenerative diseases or any neuropathy.
4. With hematologic diseases or blood coagulation disorder.
5. With hepatic or renal dysfunction.
6. With ongoing or active infectious diseases.
7. With traumatic brain injury.
8. Non-traumatic SCI caused by spinal tumors, myelitis, demyelination or spinal vascular malformation.
9. Pregnancy or lactation women.
10. Psychiatric, addictive or any other disease that compromises ability to give a truly informed consent.
11. Predicted lifespan of less than 12 months following the end of hUC-MSCs transplantation.
12. Any medical condition that, in the opinion of the investigators, may cause a safety risk to participants in this study, confound safety or efficacy assessments, or interfere with study participation.
If any clause of the exclusion criteria is met, the participant will be removed.
The rejection criteria are as follows:
1. Misdiagnosis.
2. Use of any medication that may significantly impact the assessment accuracy of hUC-MSCs transplantation.
3. Absence of any evaluation outcome at any time point during the follow-up period.
4. Previous history of participating in any other stem cell-associated clinical study or currently participating in other associated studies.
For any rejected subject, the reasons for rejection will be explained, and a case report form (CRF) containing the discontinuation date will be filed.
The cessation criteria are as follows:
1. Participant’s preference.
2. Emergence of any hUC-MSCs-related serious adverse events (SAEs) that may worsen neurological dysfunction, affect mental status, pose a life-threatening risk or result in death in any participant.
3. Identification of any significant error in the current study protocol during its execution.
4. Inability to execute the current study protocol by investigators.
5. The national regulatory authority mandates the suspension of the present clinical study.
Intervention
In this study, intrathecal transplantation of hUC-MSCs is the intervention factor. Specifically, all 43 participants will receive four times of subarachnoid delivery of hUC-MSCs with the interval time of one month.
hUC-MSCs preparation
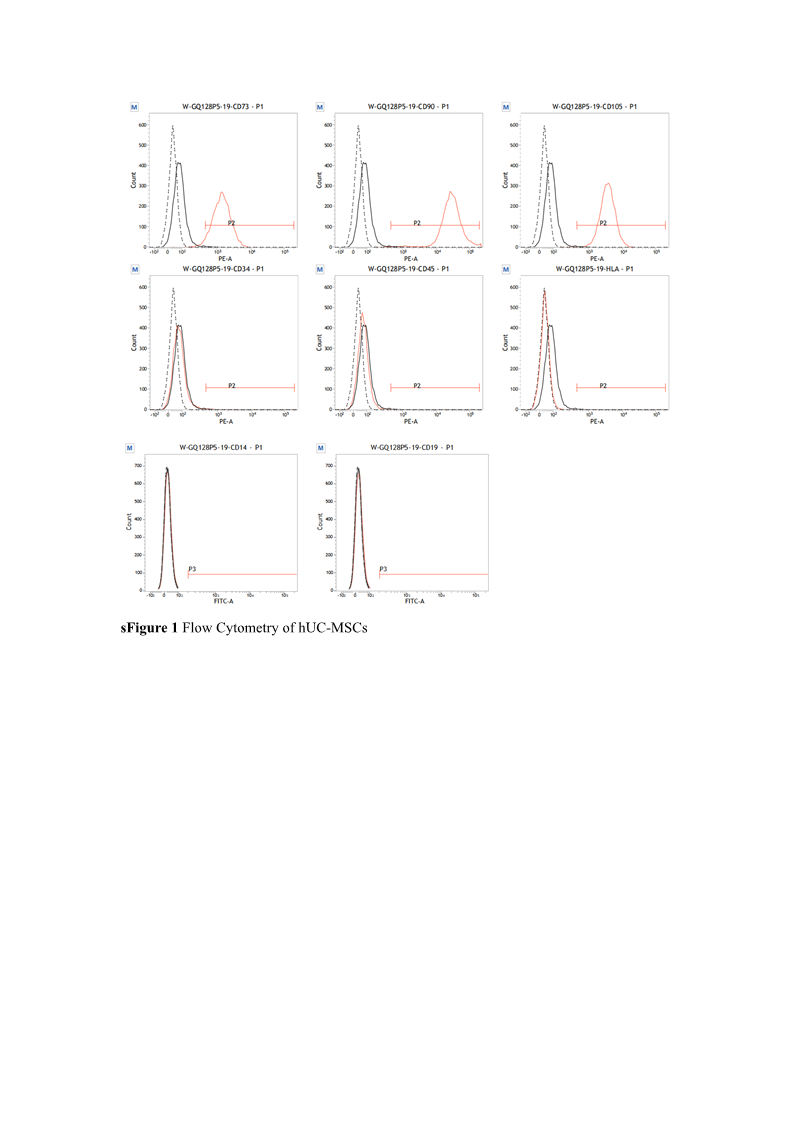
The hUC-MSCs will be manufactured in a Good Manufacturing Practice-compliant laboratory. The isolation and expansion of hUC-MSCs will be carried out through a series of steps. Upon obtaining informed consent from the parents of healthy full-term neonates, the umbilical cords will be collected, segmented, disinfected, and rinsed with sterile saline. After excising the arteries and vessels within the umbilical cord, Wharton’s jelly will be dissected into pieces smaller than 1 cm3, which will be cultured on the bottom of culture plates. Approximately one week later, cell colonies of hUC-MSCs will be visible surrounding the Wharton’ s jelly segments. Then, these primary hUC-MSCs will be dissociated using TrypLETM Express (Gibco) and then, the single-cell suspension will be adjusted to a density of 2.0×104 cells/cm2 in each plate. hUC-MSCs will be cultured in a medium composed of α-MEM (Gibco), GlutaMAXTM (Gibco) and PLUSTM MSC Qualified Cell Culture Supplement (Compass Biomedical) under a humidified atmosphere with 5% CO2 at 37℃. Upon reaching a confluence greater than 90%, the cells will be passaged to sustain continuous proliferation. A comprehensive series of quality control assessments has been conducted, including but not limited to testing for endotoxin, exotoxin, mycoplasma, chlamydia, bacterial and viral contamination, tumorigenicity, and in vitro tri-lineage differentiation potential (sTable 1-2). Additionally, cell viability and characterization of hUC-MSC surface markers were evaluated using flow cytometry performed on the BD FACSVerse™ system (sTable 3-4, sFigure 1). Based on our preclinical findings, hUC-MSCs at passages 4–5 will be administered in this clinical study at a transplantation dose of 1.0×10⁶ cells/kg26. As for transportation, sterilized hUC-MSCs will be suspended in 10 mL of sterile saline and maintained in a temperature-controlled (approximately 4℃) environment and light-protected condition. The cell suspensions will be transported as quickly as possible to ensure infusion within 8 hours of dissociation. Throughout the four-month transplantation period, all participants will receive the standard care.
Study procedure and data collection
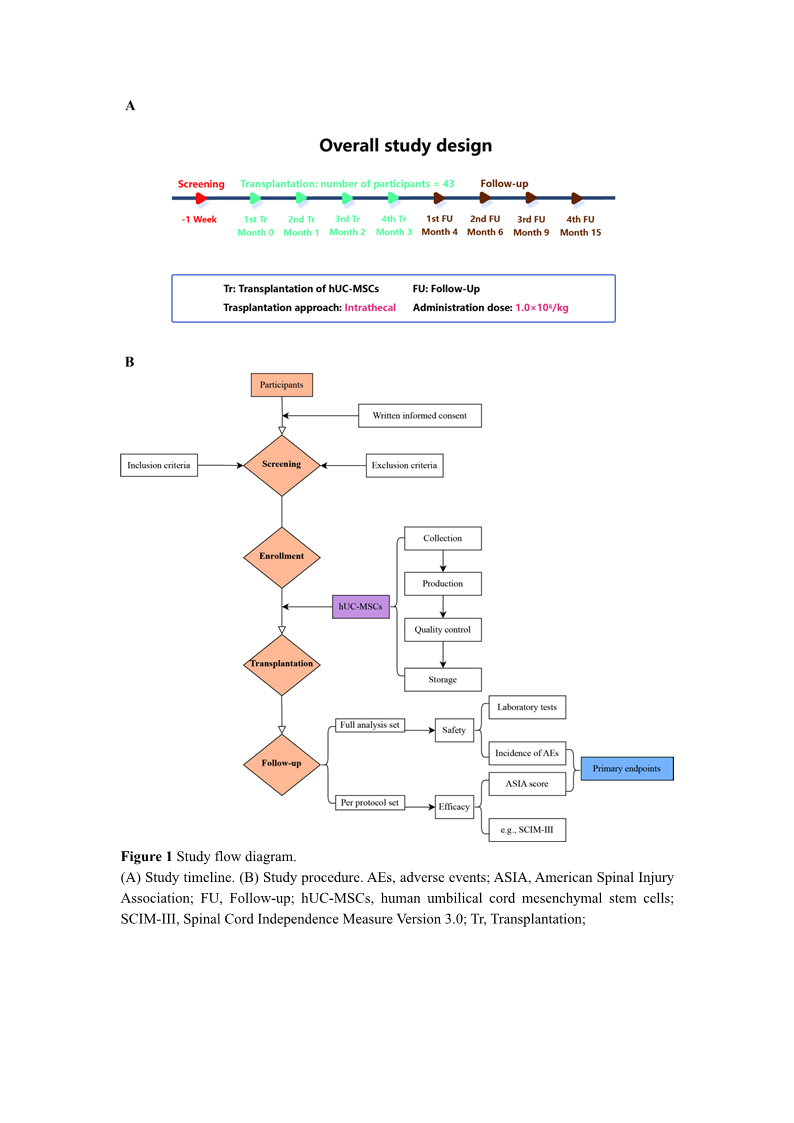
In this clinical study, each participant will receive a total of four subarachnoid infusions of hUC-MSCs once a month (Figure 1). Prior to the first hUC-MSCs infusion, baseline safety and efficacy data will be collected. During the intrathecal transplantation, each participant’s maximal lumbar flexion is sustained, and approximately 10 mL of cerebrospinal fluid will be released before hUC-MSCs delivery. The hUC-MSCs suspension will be manually administered at L3/4, L4/5 or L5/S1 level as slowly as possible to minimize the risk of intrathecal infusion-related complications, including headache, nausea or vomiting. One month later, participants will undergo the second intrathecal transplantation of hUC-MSCs following the acquisition of all safety and most efficacy parameters (excluding magnetic resonance imaging-diffusion tensor imaging, MRI-DTI). In accordance with this pattern, participants will receive the third and fourth rounds of hUC-MSCs infusion, with the same parameters collected as for the second administration. Following the completion of hUC-MSCs administrations, participants will be regularly followed up at four time points, scheduled at 1, 3, 6, and 12 months after final hUC-MSCs delivery. At the second follow-up visit, all safety and most efficacy indicators (excluding MRI-DTI) will be collected. For the remaining three visits, all safety and efficacy outcomes will be collected. Any participant experiencing any type of SAE, such as anaphylactic shock or central nervous system infection, will undergo immediate follow-up, and appropriate managements will be initiated as soon as possible. Unscheduled follow-ups will be continued until the participant’s condition has returned to normal. For mild or moderate adverse events (AEs), investigators will collaboratively decide whether the participant requires unscheduled follow-up visits to monitor his/her condition.
Safety assessment and management of AEs
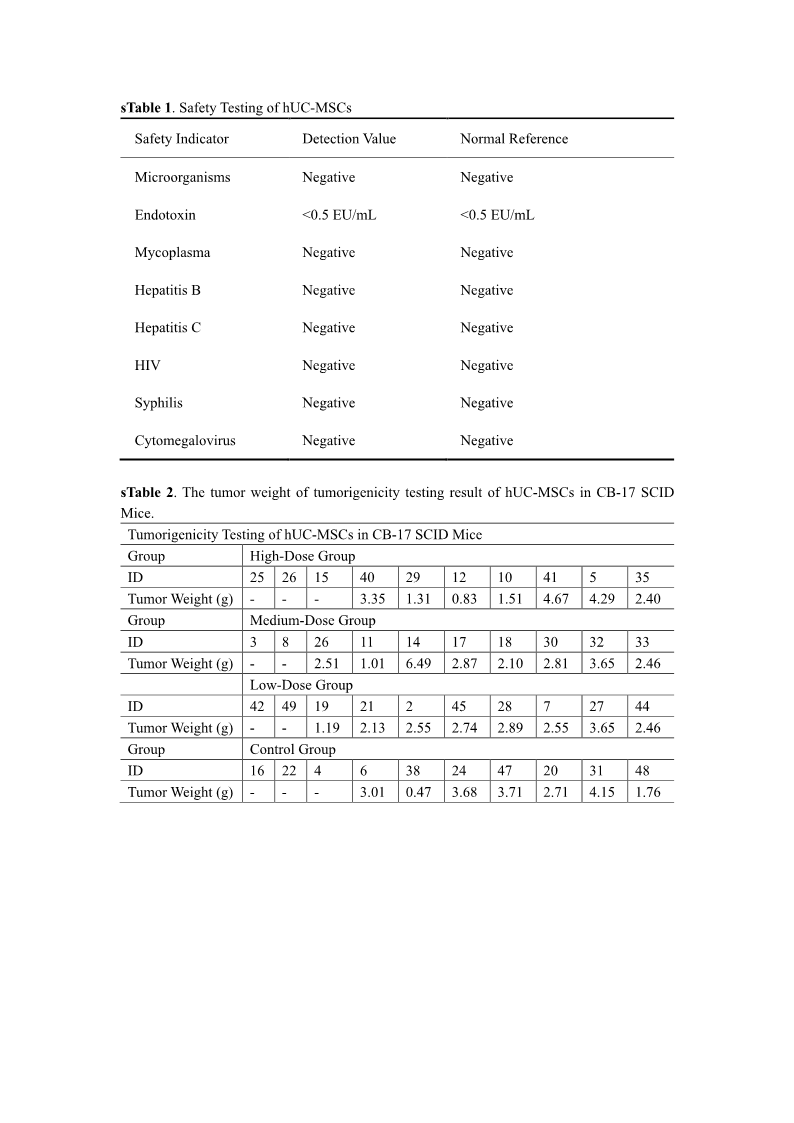
To comprehensively evaluate the safety of hUC-MSCs, a series of in vitro and in vivo assays were performed before intrathecal transplantation. In vitro tumorigenicity testing using soft agar cloning assays demonstrated that hUC-MSCs did not form any colonies over a 20-day culture period, indicating an absence of malignant transformation potential. Further, in vivo tumorigenicity studies in CB-17 severe combined immunodeficiency (SCID) mice revealed that hUC-MSCs had no significant impact on the proliferation of human lymphoma Raji tumors, reinforcing their benign nature.
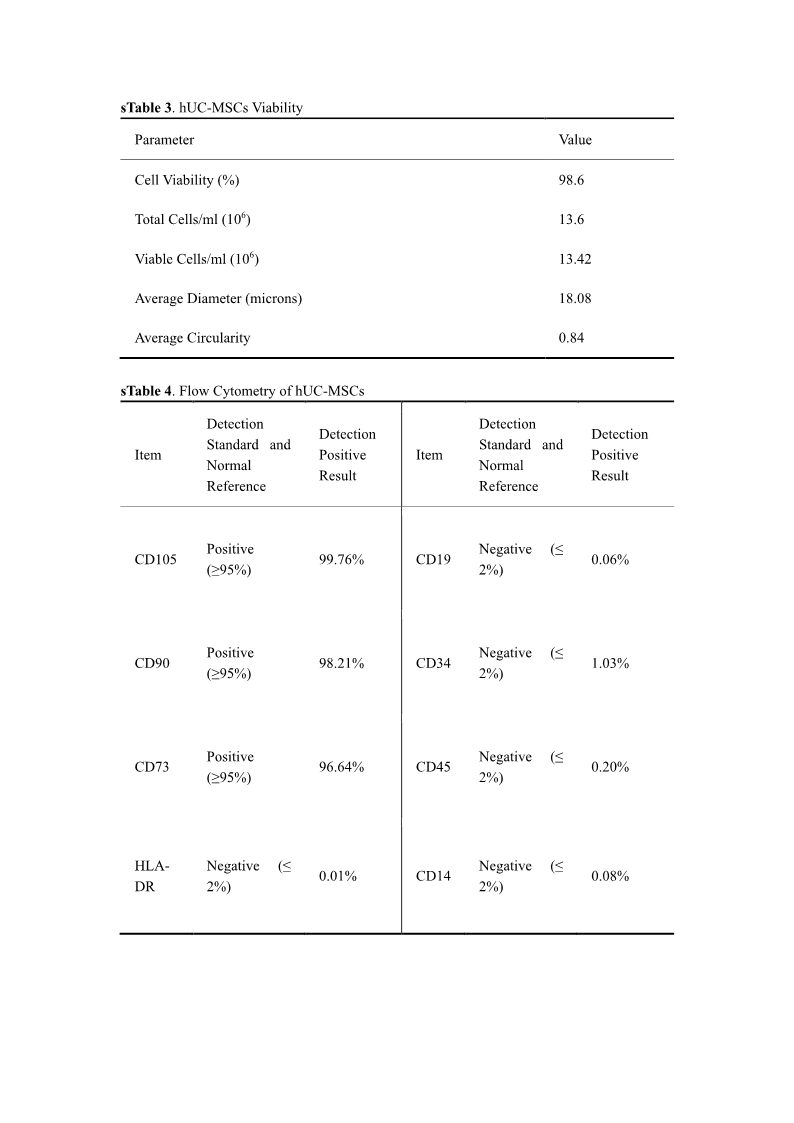
Flow cytometry analysis confirmed that hUC-MSCs exhibited characteristic surface marker associated with mesenchymal stem cells, with positive (≥ 95%) for key markers such as CD105, CD90, and CD73 and negative (≤ 2%) for hematopoietic and endothelial markers such as CD19, CD34, CD45 and Human Leukocyte Antigen-DR (HLA-DR). Moreover, safety evaluations encompassed rigorous testing for microbial contamination, endotoxins, mycoplasma and various pathogens, including hepatitis B and C viruses, HIV, syphilis and cytomegalovirus.
In this clinical study, safety of allogeneic hUC-MSC in participants suffering late chronic SCI will be assessed based on the incidence and severity of AEs. Moreover, a series of tests, including blood routine examination, urine routine examination, stool routine examination, coagulation function examination, liver and kidney function examination, tumor markers (alpha-fetoprotein, carcinoembryonic antigen, serum ferritin), chest X-ray, and electrocardiogram, will be performed.
Fever, headache, vertigo, muscle spasms, fatigue, thoracic discomfort, nausea, and vomiting are common AEs associated with hUC-MSCs delivery19–21,24. Upon identification fever, non-steroidal anti-inflammatory agents and intravenous fluids will be administered. Likewise, headaches will also be managed using non-steroidal anti-inflammatory agents. For vertigo, betahistine mesylate and flunarizine hydrochloride will be utilized to alleviate symptoms. To alleviate muscle spasms, muscle relaxant will be given. In cases of fatigue and thoracic discomfort, recommendations for bed rest and intermittent oxygen inhalation will be provided. For the management of nausea and vomiting, intramuscular injections of metoclopramide or ondansetron will be administered. Should any SAE occur, regardless of its low incidence, it will be reported to the principal investigator, the stem cell research ethics committee, and the relevant governmental supervision agency within 24 hours after its occurrence. All AEs will be coded according to the World Health Organization Adverse Reactions Terminology. Upon completion of this clinical study, the intensity and relationship of any AEs with the study intervention will be identified.
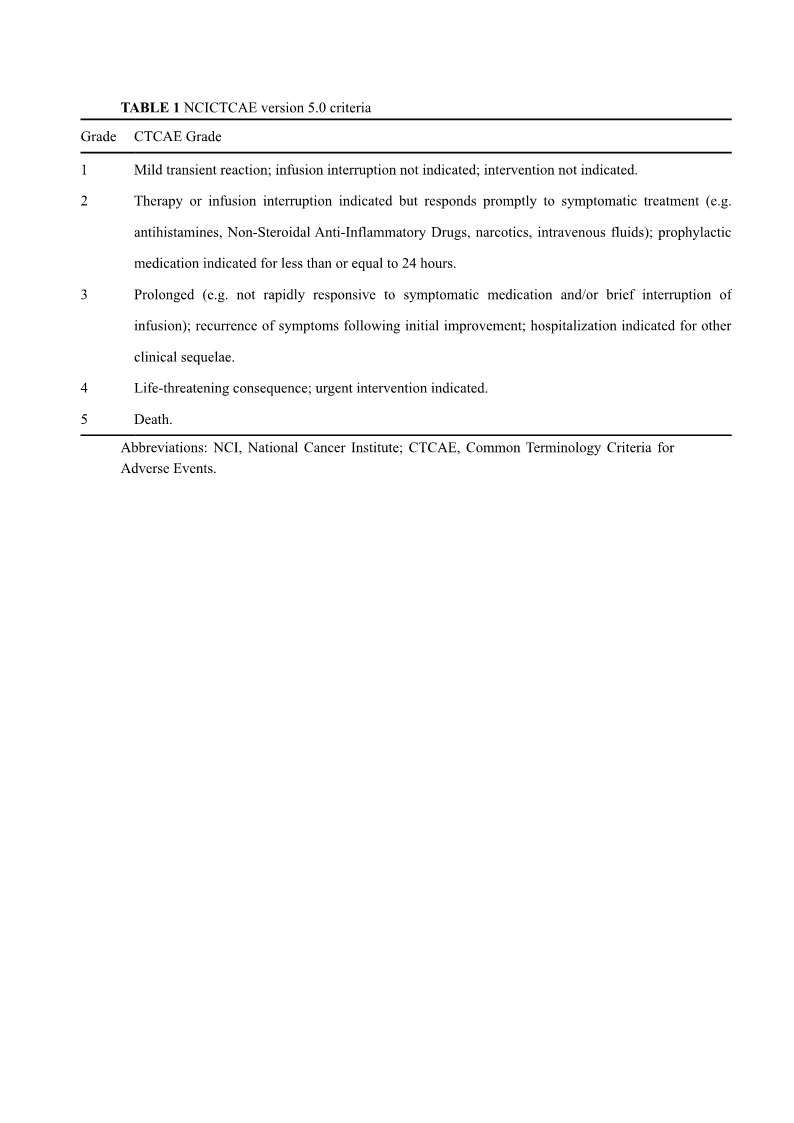
The severity of AEs should be evaluated based on the NCICTCAE version 5.0 criteria33, as outlined in the Table 1, and the CTCAE Grade 4-5 is considered as SAE in this clinical study.
Efficacy assessment
ASIA total score34,35 (range: 0-324, with lower score indicating more disability) at the fourth follow-up is the efficacy primary endpoint, whereas the scores at the other time points and additional efficacy assessments, including ASIA impairment scale (AIS), International Association of Neurorestoratology Spinal Cord Injury Functional Rating Scale36 (IANR-SCIFRS) total score (range: 0-51, with lower score indicating greater disability), Spinal Cord Independence Measure-III37 (SCIM-III) (range: 0-100, with lower score indicating greater disability), International Standards to document remaining Autonomic Function after Spinal Cord Injury38(ISAFSCI) (with more abnormal categorical items indicating greater disability; range of quantitative items: 0-28, with lower score indicating greater disability), muscle spasms assessed using modified Ashworth scale39 (range: 0-16, with higher score indicating greater disability), Penn scale40 for muscle spasticity (range: 0-4, with higher score indicating greater disability), Geffner, Gonzalez, Santacruz, and Flor scale41 (GGSF) for bladder function (range: 0-6, with lower score indicating greater disability), Neurogenic Bowel Dysfunction42 (NBD) score (range: 0-47, with higher score indicating greater disability), electromyogram (occurrence rate of F wave: range: 0-100%, with lower value indicating greater disability) , cortical sensory evoked potential (CSEP) (N9 and N20 latencies, as well as their difference: with higher value indicating greater disability), and residual urine volume (RUV) (normal range: 0-10 mL, with higher value indicating greater disability), are the secondary endpoints (Table 2).
Statistical analysis
Three different analysis sets will be established in this clinical study. The full analysis set (FAS) represents the ideal set of participants that adheres as closely as possible to the intention-to-treat principle. This set is derived from all enrolled participants, excluding those receiving no intervention or providing no evaluation outcomes. For the safety analysis set (SAS), it includes all participants who received at least once hUC-MSCs administration and is used for safety and tolerability assessments. The per-protocol set (PPS), also referred to as the efficacy subset, will be generated from participants who strictly adhere at least 2/3 fidelity of the following criteria:
1. receive a total of four hUC-MSCs administrations.
2. demonstrate no violation of the current study protocol.
3. complete the entire follow-up and obtain all necessary data.
Continuous variables will be presented as means ± standard deviations or medians with interquartile ranges depend on their normality, whereas categorical data will be reported as frequencies. For within-group comparisons, analysis of variance for repeated measures or the Friedman test will be utilized to assess overall statistical significance of continuous measures obtained at multiple (≥3) time points. After applying the Bonferroni correction, the paired t-test or Wilcoxon signed-rank test will be performed. Inter-group comparisons of continuous variables will be performed using the independent t-test or Mann-Whitney U test. Pearson’ s chi-square test or Fisher’ s exact test was employed to evaluate categorical data. All statistical analyses will be performed using Statistical Product and Service Solutions (Version 21.0, IBM, New York, NY, USA), and all statistical inferences will use two-sided tests with a significance level set at 0.05. Parameter confidence intervals will be estimated using two-sided 95% confidence intervals.
According to participant’ s characteristics, including age, disease duration, injury level and neurological dysfunction severity, subgroup analysis of the primary efficacy indicator (ASIA total scores at the fourth follow-up) will be performed.
Data management and quality control
In this clinical study, data collection will be performed using paper case report forms (CRFs). Data in the CRFs are derived from the original medical records which need to be properly preserved. The CRF of participant with an assigned number must be completed. After completion, the CRFs will be reviewed by clinical monitors before being handed over to data managers for final data entry and management. A clinical study database will be established to record all information from the CRFs. The database format will correspond as closely as possible to the CRF format to facilitate data entry. To ensure the accuracy of numerical data, double data entry by two separate operators will be performed. Data entry operators must undergo unified training and receive permissions before data entry. Also, they should follow the entry instructions and relevant standard operating procedure while entering the data. After data entry, quality control checks are required to ensure data accuracy.
Data verification will be divided into manual verification and system verification. Manual verification involves data managers detecting errors by examining consistency and logic, leading to data review queries (DRQs). System verification, or computerized edit check, refers to using computer programs to verify data in CRFs, including range, logical relationships, consistency, protocol deviations. The resulting DRQs will be handed over to clinical monitors, who will then pass them on to investigators for reconfirmation. Any modification requires the investigator’ s signature and date. After confirmation of all double-checked data and no missing queries, the database will be locked. Access to the database will be strictly limited. The principal investigator and biostatistician will have full access to the data set only with approval from the study supervisor. Data backups and paper CRF storage will be performed regularly by study coordinators. If necessary, data transfer between study centers will be encrypted, and any information that can identify individuals will be anonymized.
To ensure that this study maintains a high standard of quality and is performed in strict accordance with the current study protocol, which will only be amended in the event of SAEs during its implementation. All research personnel, including investigators, research assistants, and outcome assessors, will undergo comprehensive training prior to the trial commencement. This training will ensure their competence in administering all study procedures as outlined in this protocol. Upon initiation of this clinical study, an independent supervisor will visit to each study site monthly. The supervisor will be responsible for evaluating the overall progress and integrity of the research, adherence to the inclusion criteria for all enrolled participants, compliance with the scheduled interventions for each participant, adherence to national regulations, and the management of any practical issues that may arise. Additionally, the supervisor will periodically offer recommendations to the principal investigator, who will make the final decisions regarding any modifications, continuation, or termination of this clinical study.
Patient and public involvement
Patients and the public will not be directly involved in the formulation of scientific questions, measurement of outcomes, study design or data management.
ETHICS AND DISSEMINATION
The study ethics and study protocol have been approved by the Stem Cell Research Ethics Committee of the Third Affiliated Hospital of Sun Yat-sen University (2018-[03]) and the Ethics Committee on Stem Cell Clinical Research of West China Hospital of Sichuan University (2019-[02]), as well as by all relevant regulatory authorities. This clinical study will be performed in accordance with the principles of the World Medical Association Declaration of Helsinki, including all its amendments, and adheres to the standards of Good Clinical Practice. Once consensus on the results and conclusions of this clinical study has been reached, they will be submitted to the principal investigator and will be retained in paper form for at least 30 years. Even if the final results and conclusions do not meet the initial expectations, a manuscript describing this study will be prepared by investigators at the sponsoring institution, in strict adherence to all standard operating procedures. If investigators from the participating hospitals plan to present partial outcomes of this clinical study at academic conferences or in journals, they must obtain prior permission from the principal investigator at the sponsoring hospital. When preparing these articles, the confidentiality of all subjects will be strictly maintained.

quarterly,launched in March 2025
Editor-in-Chief: Limin Rong
Sponsor: Sun Yat-sen University
Publisher: Sun Yat-sen University Press
Co-Publisher: KeAi Communications Co., Ltd.
Edited by: Editorial Office of Journal of Brain and Spine
Address: 600 Tianhe Road, Guangzhou, 510630, China
Website: http://jbs.sypub.cn/jbs
E-mail: jbseditor@mail.sysu.edu.cn

Address:600 Tianhe Road, Guangzhou, 510630, China
Website:http://jbs.sypub.cn/jbs
E-mail:jbseditor@mail.sysu.edu.cn